These days, probably half the population has heard of weight-loss injections. Peptides like semaglutide and tirzepatide are hardly surprising anymore. Weight loss does indeed happen faster, but there’s an important detail that many people overlook. A significant portion of the weight lost isn’t fat, but muscle mass.
According to some data, muscle mass may account for up to 25-40% of total weight loss during GLP-1 therapy. In practice, this means that a person becomes smaller, but not necessarily “leaner” and sometimes even weaker and more prone to gaining fat after completing the course.
This is precisely why researchers began exploring the combination of GLP-1 drugs with GH secretagogues. To put it as simply as possible, they aim to create a formula that helps preserve and maintain muscle mass while reducing fat mass. But does it really work?
Important: Although GLP-1 agonists are FDA-approved medications, they should only be prescribed and used by a qualified physician after a thorough evaluation of your specific case. GH secretagogues remain investigational compounds. The material below describes existing approaches and the rationale for combining them, but it is not a medical recommendation or treatment protocol. Any use of medications that affects your health must be under medical supervision.
Does Semaglutide Cause Muscle Loss? The Problem Explained
Does semaglutide cause muscle loss? To be honest, yes, to a certain extent. A loss of muscle mass accompanies any rapid weight loss, and GLP-1 agonists, such as semaglutide, cause weight loss so rapidly that it becomes noticeable.
Studies on semaglutide often cite a figure of around 25-40% of total weight loss attributable specifically to lean body mass, rather than just fat. The mechanisms here are quite clear: a marked reduction in appetite often leads to insufficient protein intake. Additionally, using the drug creates a sharp calorie deficit that forces the body to use muscle as an energy source.
Semaglutide muscle loss is not just a statistic; it has practical consequences: muscle mass directly affects metabolic rate (the less muscle you have, the easier it is for fat to return), and it is also critically important for strength and functionality, especially as we age. The drug is excellent for weight loss, but without specific efforts to preserve muscle, a person risks ending up with a result that is “less on the scale but worse in terms of muscle-to-fat ratio” than originally desired.
Semaglutide vs Tirzepatide Muscle Loss – Which Is Worse?
The question of semaglutide vs. tirzepatide muscle loss naturally arises for those choosing between the two drugs (use must be supervised by a qualified professional!). Both lead to a loss of lean body mass as part of significant weight loss, but there are nuances.
Tirzepatide is a dual GLP-1/GIP receptor agonist. This means it typically results in greater overall weight loss than semaglutide, which may, in turn, reflect greater absolute muscle mass loss simply due to the larger volume. At the same time, some data suggest that the GIP component of tirzepatide may have a slightly more favorable effect on body composition, potentially preserving a slightly better ratio of lean body mass to fat mass.
Looking at the bigger picture, the tirzepatide vs semaglutide muscle loss picture looks like this: both drugs, without additional measures to preserve muscle, lead to a noticeable loss of lean body mass. The difference between them is, in itself, significantly smaller than the difference created by the individual’s own actions (protein intake and strength training). The choice between drugs should be based primarily on a specialist’s recommendations, efficacy, cost, and tolerability, with the understanding that muscle preservation depends far more on the accompanying protocol than on the choice of a specific GLP-1 drug.
How GH Secretagogues Preserve Muscle During Fat Loss
GH secretagogues (CJC-1295, ipamorelin, sermorelin, tesamorelin) counteract muscle loss caused by GLP-1 through a complementary mechanism. These peptides amplify natural growth hormone pulses, which stimulate protein synthesis, support the preservation of lean body mass, and primarily “draw” energy from fat stores, leaving muscles relatively untouched.
Some studies suggest that, when combined with a GLP-1 drug, a GH secretagogue helps shift the body’s metabolism toward fat utilization. As a result, GLP-1 promotes fat loss, while the GH secretagogue helps preserve (and, with exercise, even slightly increase) muscle mass. Additionally, GH secretagogues are associated with improved sleep quality, and it is during sleep that a significant portion of muscle recovery and growth hormone production occurs. However, this is only preliminary research, and there is still no definitive data. Making independent decisions about using any of these peptides is clearly unwise, given the unknown long-term effects on your body.
The Best Peptide Stack for Muscle Growth and Fat Loss
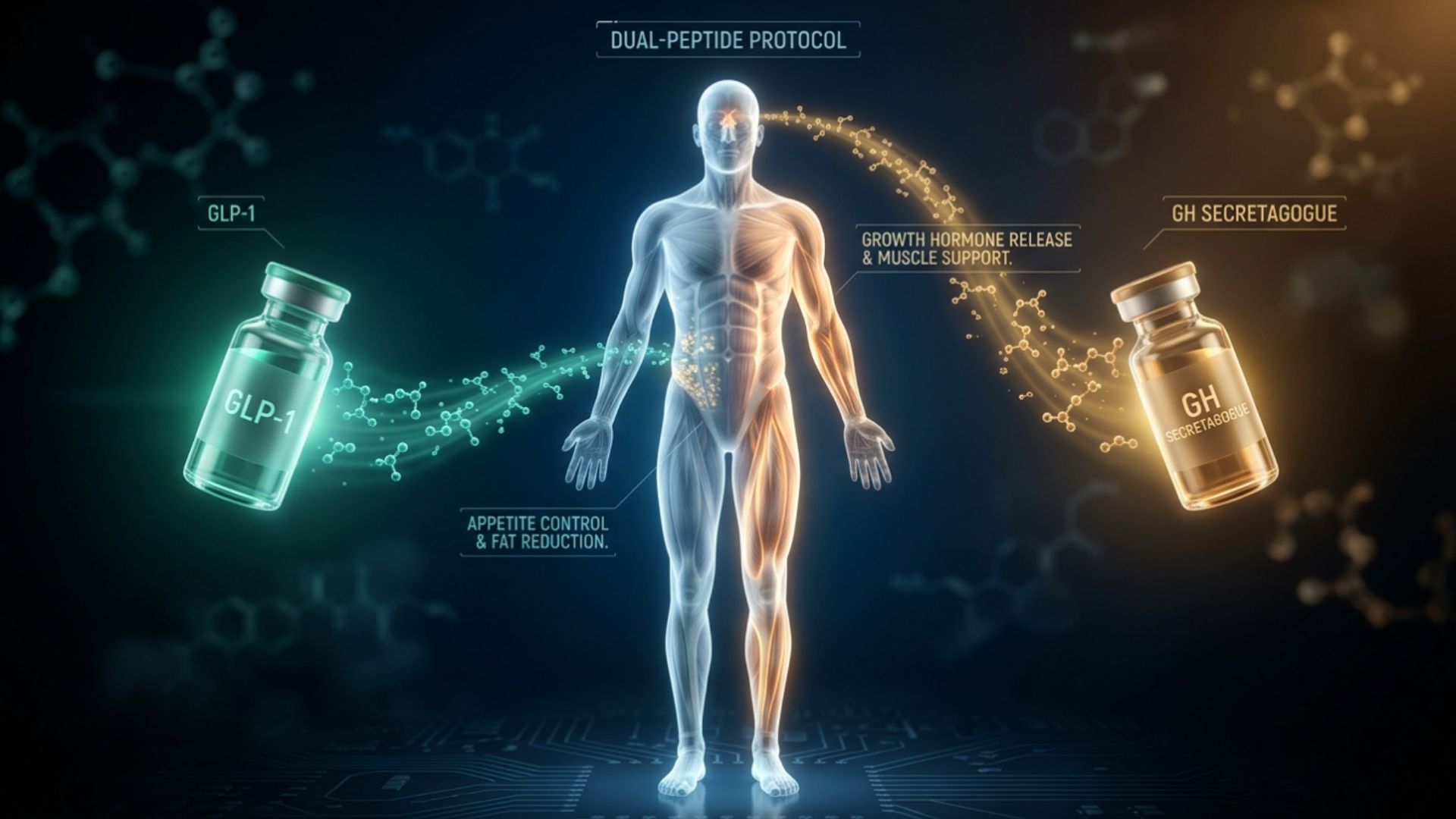
The best peptide stack for muscle growth and fat loss is based on a combination of a GLP-1 agonist and a GH secretagogue – this allows you to work on both aspects of body recomposition simultaneously. The core of this approach: a GLP-1 drug (semaglutide or tirzepatide) to control appetite and reduce body fat, combined with CJC-1295/ipamorelin to preserve muscle, support recovery, and optimize growth hormone production.
The GLP-1 component addresses calorie deficit and fat loss, while the GH secretagogue preserves lean body mass, improves recovery, and supports the body’s ability to maintain and build muscle through training. Some protocols also mention BPC-157 – to support recovery during a calorie deficit (training in a deficit increases the risk of injury) – and sometimes tesamorelin due to its specific effect on visceral fat.
The best peptides for fat loss and muscle gain work (in the early stages of research; there is still no large-scale official data) precisely because they address the opposing goals of body recomposition: one component removes fat, while the other protects and supports muscle. This is fundamentally different from using GLP-1 alone – the peptide stack for muscle growth and fat loss transforms simple weight loss into true body recomposition – that very “leaner” and stronger physique people usually strive for, rather than just a lower number on the scale.
Dosing the Stack – GLP-1 and GH Secretagogue Protocols
In general terms, the best peptide stack for weight loss while preserving muscle involves coordinating two distinct “regimens.” In clinical practice, the GLP-1 component is titrated gradually – the dose is increased over several months (as reported in studies). This allows for the management of gastrointestinal side effects. GH secretagogues are usually taken daily, often before bed, to enhance the natural nighttime surge of growth hormone.
However, the peptides themselves are only part of the picture. Without the following elements, even a well-designed peptide stack for muscle growth and fat loss performs significantly worse:
- Adequate protein intake is a critical factor for preserving muscle mass during a calorie deficit.
- Regular strength training is what signals the body to preserve muscle rather than use it as an energy source.
- Quality sleep, since most of the restorative and hormonal effects occur during sleep.
When prescribed by a qualified specialist, peptides can create a suitable hormonal “environment,” but protein and exercise provide the very stimulus needed to preserve muscle. Specific regimens and dosages must be determined on an individual basis, in consultation with a doctor, taking into account your health status and any medications you are taking.
Best Peptide Stack for Weight Loss for Women
The best peptide stack for weight loss for women follows the same “GLP-1 plus GH secretagogue” logic, but with some nuances. Women generally respond well to more conservative doses of GH secretagogues compared to those used in male protocols, and even such mild regimens ensure effective muscle mass preservation without unwanted side effects. At the same time, women are particularly vulnerable to muscle loss on GLP-1 therapy, as they generally have less muscle mass to begin with than men.
The female version of body recomposition usually results in a more defined, toned physique rather than “bulk” – a common but unfounded fear. Protein and strength training are just as important for women as they are for men. The fear of “bulking up” often leads to insufficient training and inadequate protein intake, which ultimately sabotages muscle preservation during weight loss.
Realistic Results and How to Track Body Composition
The combination of fat loss and muscle preservation yields results that the scale doesn’t show, which is precisely why tracking progress matters here.
With the right combination of adequate protein and training, fat loss typically occurs steadily, while muscle mass is preserved or even increases slightly. This means the body becomes more defined. Key point: the number on the scale may change more slowly than with GLP-1 monotherapy, simply because muscle is preserved (and muscle is denser than fat, so it takes up less space for the same weight), but the final result in terms of body composition is significantly better.
Therefore, it makes more sense to focus not on weight, but on body composition metrics – body fat percentage, progress photos, strength metrics, and how clothes fit. In terms of timing, fat loss usually begins in the first few weeks as GLP-1 takes effect. In contrast, the effects of GH secretagogues on muscle recovery and preservation become apparent within a few weeks. Noticeable body recomposition becomes visible after a few months. Patience and proper progress tracking help avoid a common mistake: evaluating results solely by the scale, which devalues the very muscle preservation that makes this approach more valuable than GLP-1 alone.
Is This Stack Right for You? Safety and Practical Takeaways
This approach is most relevant for those taking GLP-1 medications who are concerned about losing muscle along with fat, for those specifically aiming for body recomposition rather than just weight loss, for people over 40 (when muscle loss is harder to compensate for later), and for anyone who wants to maintain their metabolism over the long term.
This approach is less suitable for athletes undergoing doping tests (GH secretagogues are on the WADA/USADA lists of prohibited substances), for those who are not ready to commit to protein intake and strength training (without this, even a well-designed stack works significantly less effectively), as well as for people with a history of cancer, for whom GH secretagogues require special caution.
From a safety perspective, GLP-1 drugs can cause gastrointestinal side effects and come with a class warning regarding the risk of thyroid tumors; GH secretagogues can affect fluid retention, insulin sensitivity, and cause symptoms similar to carpal tunnel syndrome.
To sum it up: the combination of GLP-1 and GH secretagogues is a strategy in which one addresses fat loss and the other addresses muscle preservation, provided that protein, training, and sleep remain the foundation on which both components rely. Peptides for fat loss and muscle gain in this context are about turning weight loss into a true body composition transformation, rather than just a lower number on the scale.
Important. All peptides mentioned in this text are provided for informational purposes only. The final decision regarding their use, as well as the selection and combination of any weight-loss supplements, must be made by a qualified specialist, taking into account the individual’s health status, medical history, and current medications.