
What Is Thymosin Alpha-1? Immune Function, Benefits, and Research Overview
Last Updated: May 30, 2026
Medically Reviewed by: Dr. Sarah Mitchell, MD, Board-Certified Immunologist
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Thymosin alpha-1 is considered a research peptide in many jurisdictions and should only be used under the supervision of a qualified healthcare provider. Consult your physician before beginning any peptide therapy protocol.
“Thymosin alpha-1 is one of those peptides where the science genuinely precedes the hype — it has over five decades of published research behind it, which is rare in this space. Our job is to help people separate what’s been demonstrated from what’s been assumed.” — Rusty Ryan, Iron Peptides
TL;DR: Article Summary
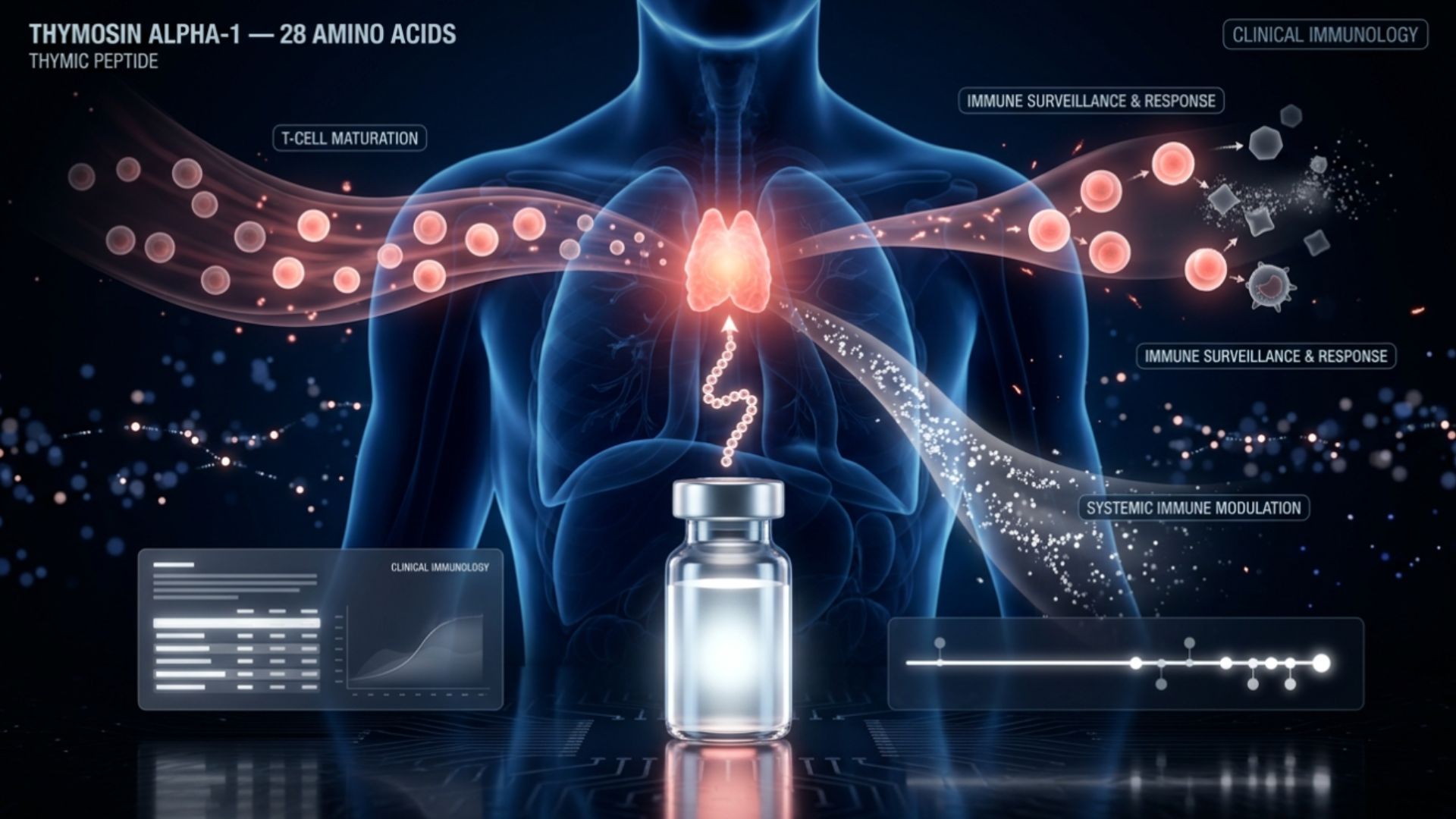
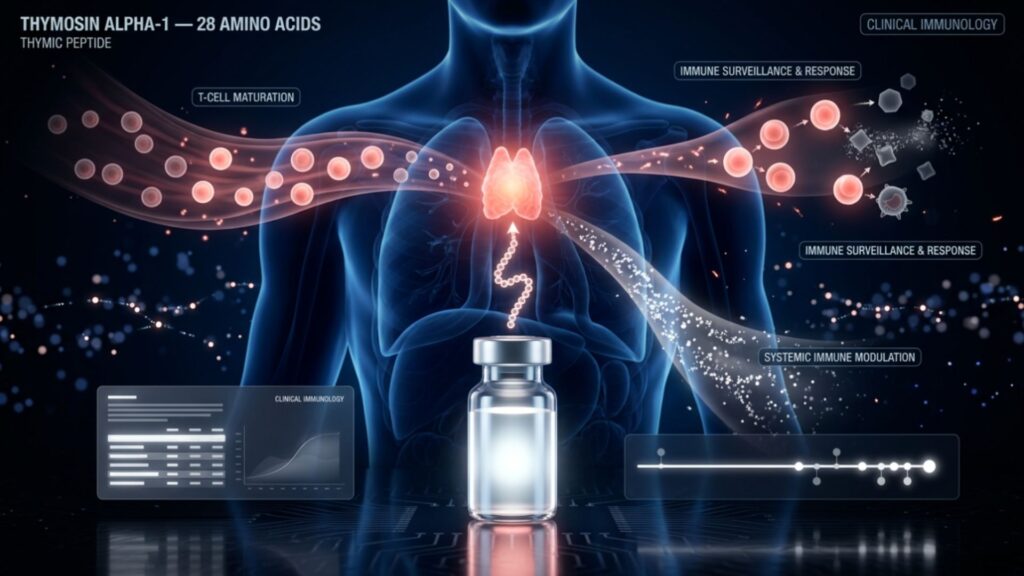
- What it is: Thymosin alpha-1 (TA1) is a 28-amino-acid immunomodulatory peptide naturally produced by the thymus gland.
- Mechanism: It acts as an immune “normalizer,” enhancing dendritic cell maturation and shifting T-cells toward a Th1 profile.
- Key Benefits: Strongest evidence supports use in severe viral infections, sepsis, and critical care scenarios.
- Standard Dosage: 1.6 mg injected subcutaneously twice weekly is the most researched protocol.
- Safety: Generally robust safety profile; not FDA-approved in the US but approved in 35+ other countries as Zadaxin®.
What Is Thymosin Alpha-1 and How Does It Work?
Thymosin alpha-1 (TA1) is an immune system “normalizer.” Unlike stimulants that cause indiscriminate inflammation, TA1 upregulates cellular immunity when suppressed and promotes regulatory pathways when inflammation is too high. It coordinates interactions between antigen-presenting cells, T-cells, natural killer (NK) cells, and macrophages.
Origin and Biochemistry
Isolated in 1977 by Low and Goldstein, TA1 is a discrete 28-amino-acid molecule.
- Sequence: Ac-Ser-Asp-Ala-Ala-Val-Asp-Thr-Ser-Ser-Glu-Ile-Thr-Thr-Lys-Asp-Leu-Lys-Glu-Lys-Lys-Glu-Val-Val-Glu-Glu-Ala-Glu-Asn.
- N-terminal acetylation: Critical for its function.
- Half-life: Relatively short (2–4 hours in humans), which is why subcutaneous injection is the preferred delivery method.
How TA1 Modulates the Immune System
- Dendritic Cells: Enhances antigen presentation, bridging innate and adaptive immunity.
- T-Cell Differentiation: Promotes Th1 phenotypes (IFN-γ production) while supporting Regulatory T-cells (Tregs) to maintain tolerance.
- Cytokine Regulation: Increases IFN-γ while reducing TNF-α in cases of sepsis.
- NK Cells: Increases cytotoxicity by 30–50% to better fight infected or malignant cells.
Benefits Supported by Research
Antiviral and Anti-Infection Applications
- Hepatitis B: Research shows TA1 combined with interferon-alpha significantly improved clearance of HBV DNA compared to interferon alone.
- Hepatitis C: Historically used, though modern direct-acting antivirals have largely replaced it.
- Sepsis: TA1 is highly active in sepsis research, with studies showing a reduction in 28-day mortality rates by addressing immune paralysis.
Emerging Data: COVID-19 and Severe Acute Pancreatitis
- COVID-19: Used to combat cytokine storms and T-cell exhaustion in severe cases.
- Severe Acute Pancreatitis (SAP): 2025 meta-analysis showed TA1 significantly reduced secondary infections and C-reactive protein (CRP) levels.
Oncology and Autoimmune Support
- Oncology: Studied as an adjunct to chemotherapy to mitigate treatment-induced immunosuppression (e.g., in lung and liver cancers).
- Autoimmune: Theoretical potential to balance T-cell profiles, though the evidence base remains small.
Dosage Protocols
Note: These are based on clinical research protocols, not medical prescriptions.
| Scenario | Typical Dose | Frequency | Route | Duration |
| Maintenance/Support | 1.6 mg | Twice weekly | Subcutaneous | 4–24 weeks |
| Acute Illness (Sepsis) | 1.6 mg | 1–2x Daily | Subcutaneous | 5–14 days |
| Oncology Adjunct | 1.6 mg | Twice weekly | Subcutaneous | Cycle duration |
Side Effects and Safety
TA1 is noted for having a very favorable safety record across thousands of patients.
- Common: Injection-site reactions (redness/itching in 15–25% of users).
- Rare: Headache, transient low-grade fever, or mild nausea.
- Interactions: Does not interfere with the cytochrome P450 pathway, making it safe to use with many other medications.
Regulatory Status and Sourcing
- Zadaxin®: The pharmaceutical version is approved in 35+ countries.
- FDA Status: Not FDA-approved for use in the USA.
- Sourcing: Often sold as a “research chemical.” Buyers should demand HPLC and Mass Spectrometry results verifying >98% purity to avoid heavy metals or endotoxin contamination.
Thymalin vs. TA1
- Thymalin: A bovine thymus extract; composition varies batch-to-batch.
- Thymosin Alpha-1: A synthetic, single-entity peptide with high consistency and a robust modern evidence base.
Frequently Asked Questions
How long before I see results?
Cellular changes occur within 10–14 days, but clinical benefits for chronic conditions are typically measured over 3–6 months.
Is it legal?
In the US/UK, it is legally sold only as a “research chemical” for laboratory use. Human self-administration exists in a legal grey area.
Can I use it with an autoimmune condition?
Medical supervision is mandatory. While it can support tolerance, it also pushes Th1 profiles, which might exacerbate specific conditions.
Is the nasal spray effective?
Efficacy is unestablished compared to injections. As a large hydrophilic peptide, TA1 does not cross mucosal barriers easily without specialized carriers.
Who should avoid it?
Pregnant/breastfeeding women, children, and organ transplant recipients (risk of organ rejection).
Related Articles

Updated: May 30, 2026 Reviewed by: Rusty Ryan, Lead Formulation Specialist at Iron Peptides. “Most people researching
- June 23, 2026
Last Updated: May 30, 2026 Medically Reviewed by: Dr. Sarah Mitchell, MD, Board-Certified Immunologist Medical Disclaimer: This
- June 22, 2026
MEDICAL DISCLAIMER: This article is for educational and informational purposes only. It does not constitute medical advice,
- June 21, 2026